J Atherosclerosis Prev Treat. 2022 Jan-Apr;13(1):17-25 | doi:10.53590/japt.02.1030
REVIEW ARTICLE
Evangelia S. Makri, Stergios A. Polyzos
First Laboratory of Pharmacology, School of Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece
![]()
Abstract
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease affecting millions of people worldwide with potentially serious complications that may lead to mortality and constitute a significant socioeconomic burden. Although modern lifestyle, obesity and insulin resistance play leading roles in the pathophysiology of the disease, various metabolic aberrations, as well as genetic predisposition participate in the development and progression of NAFLD. The diagnosis of NAFLD, especially the early recognition of NASH and fibrosis, is vital for the early management of the disease. Many diagnostic methods have been developed for the disease, ranging from liver biopsy to imaging techniques and serum biomarkers, each one followed by advantages and disadvantages. Despite the extensive research in this field, there is to-date no licensed pharmacological treatment. However, several medications have been investigated and provided promising results; in this regard, the results of some phase III clinical trials in NASH patients are expected. Until the approval of specific for the disease medications, the cornerstone of its management remains lifestyle modifications, i.e. dietary changes and increase in physical activity.
Key words: Diagnosis, fibrosis, nonalcoholic fatty liver disease, nonalcoholic steatohepatitis, pathophysiology, treatment
Corresponding author: Evangelia S. Makri MD, MSc, cPhD, First Laboratory of Pharmacology, School of Medicine Campus of Aristotle University of Thessaloniki 54 124, Thessaloniki, Macedonia, Greece, Tel.: +30 2351046216, e-mail: evi-mak@hotmail.com
Submission: 25.11.2021, Acceptance: 05.02.2022
INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease with an increased prevalence over the last few years, estimated to be 25% worldwide1. The phenotypes of NAFLD include simple steatosis (nonalcoholic fatty liver; NAFL), which is characterized by lipid accumulation in the hepatocytes, and nonalcoholic steatohepatitis (NASH), which is characterized by inflammation and hepatocellular damage2. NAFL may progress to NASH in a subset of patients, and, subsequently, NASH may progress to hepatic fibrosis, cirrhosis and even hepatocellular carcinoma in a minority of patients1.
Multiple risk factors have been implicated in the development and progression of NAFLD, including components of the metabolic syndrome, e.g., obesity, type 2 diabetes mellitus (T2DM), dyslipidemia, as well as variable stressors, environmental factors, microbiota and genetics3-5. Recently, an expert panel published a consensus recommending a new nomenclature for NAFLD6. The suggested term, metabolic (dysfunction)-associated fatty liver disease (MAFLD), is directed towards a diagnosis based on certain criteria, rather than the exclusion of other liver diseases (e.g., alcoholic liver disease, viral hepatitis etc.) followed at the diagnosis of NAFLD7. Promising though, there is an ambiguity about the new term, which places the disease in its metabolic milieu, but there are several issues that need to be resolved8. NAFLD is also considered a multi-systemic disease, as it accompanies extra-hepatic co-morbidities, such as cardiovascular disease, chronic kidney disease and various types of malignancies, thus contributing to all-cause mortality increment9-11.
Lifestyle modifications, mainly a combination of weight reduction and exercise, have been proposed for the management of NAFLD2,12. Even minimal weight loss renders appreciable decrease in insulin resistance (IR) and hepatic fat12. However, the majority of patients fail to comply with these recommendations in the long-term13. Despite the increased prevalence and possible fatal consequences connected to NAFLD, pharmacological treatment is yet an unmet need: extensive effort with a large number of clinical trials attempted to unravel the medication(s) that could potentially prevent NAFLD and/or lead to the regression of the advanced disease13. Although a variety of existing medications has also been investigated in the treatment of NAFLD, including antioxidants, anti-diabetics, cytoprotective agents, bile acids, none of them has been officially approved as yet14.
The aim of this review is to provide a synopsis of the key points of the pathogenesis, diagnosis and treatment of NAFLD.
PATHOPHYSIOLOGY
The pathophysiology of NAFLD is considered multi-factorial and various mechanisms have been proposed. The previously suggested “two-hit hypothesis” emphasized in a first hit (factor) leading to hepatic steatosis, followed by a second hit leading to hepatic inflammation and fibrosis15. The above hypothesis has been replaced by the “parallel multiple-hit hypothesis”, supporting that several “hits” contribute simultaneously to the development and progression of NAFLD16; in this regard, NAFLD is a dynamic disease that is affected by ever changing factors in an individual basis17.
As mentioned above, NAFLD is characterized by the presence of lipid accumulation in the hepatocytes, in the form of triglycerides (TGs). The main sources of free fatty acids (FFAs), which are esterified to TGs in the liver, are lipolysis in the adipose tissue, de novo lipogenesis in the hepatocyte, and dietary intake18. When FFAs influx overwhelms their utilization and the storing capacity of the hepatocytes, the accumulation of TGs into the hepatocytes results in lipotoxicity, hepatocellular injury, oxidative stress and intra-hepatic inflammation, which highlight the progression to NASH4,19. Further liver damage leads to cell apoptosis and a failure to the mechanisms of regeneration, which highlight the progression to fibrosis and even to cirrhosis, the end stage of fibrosis.
Among the fundamental factors, a high-calorie diet, in parallel with a sedentary lifestyle, has been associated with NAFLD. The abundance mainly of carbohydrates and fats on dietary habits contributes to NAFLD, either in a direct manner or indirectly, through body weight increment9. Excess calorie intake, in combination with increased lipolysis, owing to IR, results in the storage of FFAs into ectopic fat depots, such as the liver, muscles and pancreas9,20. The dysfunctional adipose tissue, due to lipid abundance, alters the production of adipokines, thereby enhancing the inflammatory processes into the liver and favoring the progression to NASH and hepatic fibrosis21.
In this regard, obesity is considered to be a major driver of the development and progression of NAFLD9. Although obesity constitutes a potent factor in the development of NAFLD, evidence from a meta-analysis showed that among NAFLD patients, 40% were non-obese and 19% were lean, confirming the contribution of multiple factors in the pathophysiology of NAFLD22. IR plays a prominent role in the pathophysiology of NAFLD, which is enhanced by the increased prevalence of NAFLD in patients with T2DM and vice versa23,24. Recently, intestinal microbiota has been proposed as contributing factor to NAFLD25. Certain gut microbiota affects intestinal permeability via toxic bacterial products, thus, enhancing efflux of FFAs, bacterial translocation and inflammatory mediators, influencing liver through the gut-liver axis, thus promoting the development and progression of NAFLD26.
Apart from environmental factors, genetic variations also contribute to NAFLD pathogenesis27. Among various genetic polymorphisms resulting in impaired metabolism of liver lipids and consequently, NAFLD, the genetic variant rs738409 in the patatin-like phospholipase domain-containing protein 3 (PNPLA3) gene, constitutes the most validated genetic determinant of NAFLD28. Other important genetic variations associated with NAFLD refer to transmembrane 6 superfamily member 2 (TM6SF2), membrane bound O-acyltransferase domain-containing 7 (MBOAT7) and glucokinase regulator (GCKR) genes27. It also seems that NAFLD is associated with ageing, since its prevalence increases with advanced age independently from the increase in body weight1.
By identifying the mechanisms of the disease, new opportunities are revealed on the early recognition of the individual risk to present NAFLD and thus tailored treatments may be developed in a personalized basis.
DIAGNOSIS
Τhe bridge between the etiology of a disease and the appropriate treatment is the correct and definite diagnosis of the individuals affected by the disease. In terms of NAFLD, the inherent disease complexity and the wide phenotypic spectrum dictate the need for an accurate diagnostic tool, so that patients can be properly categorized, before scheduling the appropriate management. Key points in the diagnosis of NAFLD remain the discrimination of simple steatosis from NASH and the recognition of advanced fibrosis.
Liver biopsy remains the “gold standard” method to assess the grade and the severity of NAFLD29. The most commonly used histological system is currently the NAFLD activity score (NAS)30. NAS assesses steatosis grade, lobular inflammation and ballooning and represents an established tool. Except for NAS, fibrosis stage is important to be determined, since this is the main histological prognostic factor of advanced disease and a difficult to treat target31. Nonetheless, liver biopsy has several limitations, since it is an invasive method with scarce, but existing complications and mortality, it has sampling error, inter-observer variability, restricted patient consent and high cost, which render the need for the development of noninvasive diagnostic tools of importance32.
Noninvasive tools are based on imaging and/or serum biomarkers. Among imaging techniques, ultrasonorgaphy (US), an inexpensive, widely available and safe tool, presents the lowest sensitivity and specificity, whereas, computed tomography (CT) demonstrates better specificity, although radiation exposure remains a notable drawback33. Notwithstanding, US is recommended by all guidelines as the first step diagnostic tool, albeit it can predict NAFL only when hepatic lipid content is more than 12.5-20%2,33. Magnetic resonance (MR) imaging (MRI) and spectroscopy (MRS) are considered to have substantial sensitivity and specificity, without variability and radiation burden34. MRI is considered the technique of choice predicting steatosis, when liver fat content is over 5%, which represents the cut-off of NAFL diagnosis35. However, the high cost and reduced availability of these procedures eliminate their use. The above mentioned methods estimate hepatic steatosis, while for hepatic fibrosis, MR elastography (MRE) and transient elastography (TE) measure liver stiffness, considered to be an indirect index of hepatic fibrosis36,37. MRE showed better precision in identification of fibrosis stage than TE, but it is more expensive and has lower availability38.
As far as it concerns serum biomarkers, they rely on the measurement of different circulating parameters associated with liver dysfunction, inflammation or fibrosis, targeting to identify the presence of NAFLD or fibrosis. This kind of markers could derive from the measurement of a single or a combination of parameters. Current serum noninvasive indices were developed to predict not only steatosis grade (fatty liver index [FLI], NAFLD liver fat score [NAFLD-LFS], hepatic steatosis index [HSI]), but also hepatocellular apoptosis (cytokeratin-18) and fibrosis stage (NAFLD fibrosis score [NFS], fibrosis-4 index [FIB-4], aspartate aminotransferase-to-platelet ratio index [APRI])39-41. The analysis of serum indices provides the ability for rapid, inexpensive and easy diagnosis. Nevertheless, there is still a need for better validation of the existing biomarkers or search for new ones, since all the existing indices have a grey zone, i.e. indeterminate results that can neither exclude nor set the diagnosis of NAFLD or hepatic fibrosis.
The above considering, we may propose an algorithm depicted in Figure 1 for the diagnosis of NAFLD42,43. Initially, predisposing factors of NAFLD should be evaluated, including, but not limited to obesity, T2DM, metabolic syndrome and genetic predisposition. Subsequently, US and/or noninvasive indices of steatosis (e.g., FLI, HSI) may be performed and, in case of positive results, the evaluation of noninvasive indices of fibrosis (e.g., NFS, FIB-4, APRI) should be performed. If this evaluation indicates high risk of advanced fibrosis, then liver biopsy may be considered to establish the diagnosis. In case of low risk of advanced fibrosis, then follow-up every one or two years may be a reasonable approach. In case of indeterminate results, we may consider TE or MRE for further evaluation (Figure 1).
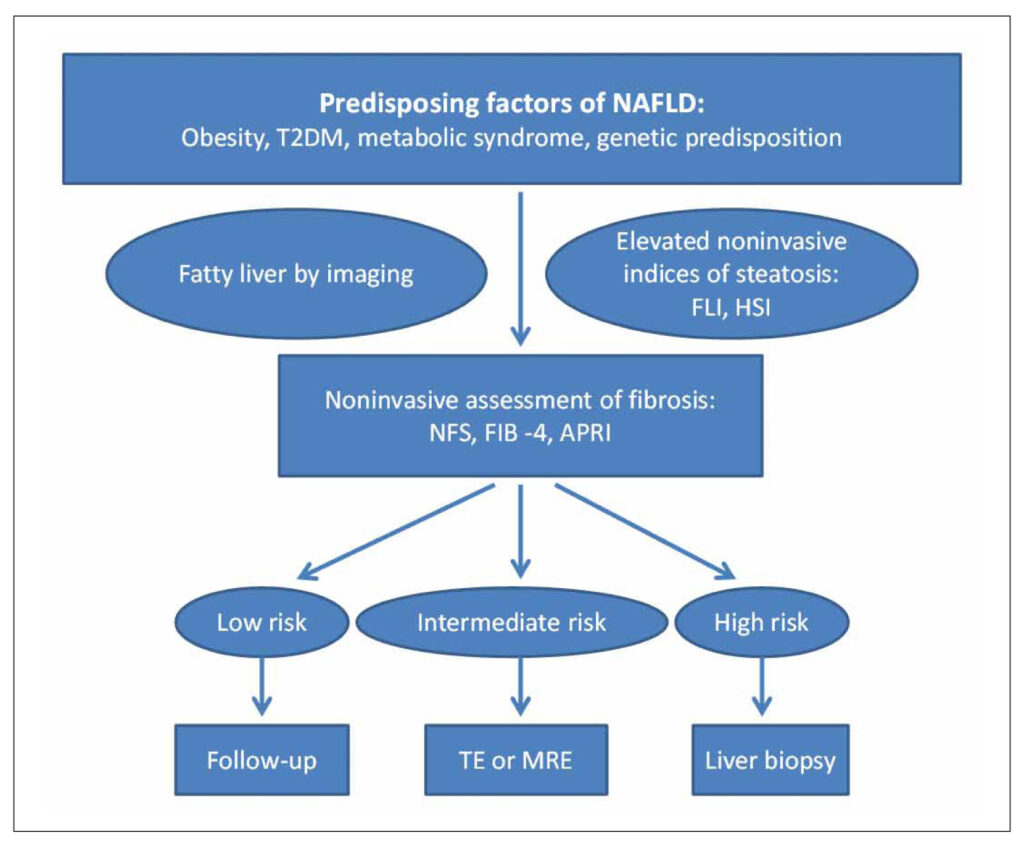
FIGURE 1. A suggested diagnostic algorithm for NAFLD. Initially, predisposing factors of NAFLD should be evaluated, including obesity, T2DM, metabolic syndrome and genetic predisposition. Subsequently, US and/or noninvasive indices of steatosis (e.g., FLI, HSI) may be performed and, in case of positive results, the evaluation of noninvasive indices of fibrosis (e.g., NFS, FIB-4, APRI) should be performed. If this evaluation indicates high risk of advanced fibrosis, then liver biopsy may be considered to establish the diagnosis. In case of low risk of advanced fibrosis, then follow-up every one or two years may be a reasonable approach. In case of indeterminate results, we may consider TE or MRE for further evaluation.
Abbreviations: ALT, alanine aminotransferase; APRI, AST-to-platelet ratio index; AST, aspartate aminotransferase; FIB-4, fibrosis-4; FLI, fatty liver index; HSI, hepatic steatosis index; MRE, magnetic resonance elastography; NAFLD, nonalcoholic fatty liver disease; NFS, NAFLD fibrosis score; TE, transient elastography; T2DM, type 2 diabetes mellitus.
TREATMENT
Treatment of NAFLD is a hot scientific field. The main therapeutic goals, adopted by most clinical trials, are currently the resolution of NASH (without worsening of fibrosis) and the improvement in fibrosis stage (without worsening of NASH). All guidelines propose lifestyle modifications as the first step for the management of NAFLD44. The proven efficacy of dietary and exercise adaptations to prevent the onset and progression of NAFLD is a yardstick against which any other treatment must be measured45,46. Additionally, as obesity is strongly associated with NAFLD, bariatric surgery in selected individuals with morbid obesity, improves hepatic steatosis, NASH and even fibrosis, which is considered a difficult therapeutic target47. Roux-en-Y gastric bypass has been proposed to be superior to the other bariatric procedures, but it is also more amputational47. Generally, body weight reduction more than 10% has shown greater rates of NASH resolution and fibrosis regression12.
Despite prominent therapeutic response with the lifestyle modifications, the poor compliance to them renders the pharmaceutical management of great importance. The investigated medications target several aspects of the pathophysiological pathways, such as metabolic aberrations, hepatic inflammation, oxidative stress and fibrosis (Figure 2).
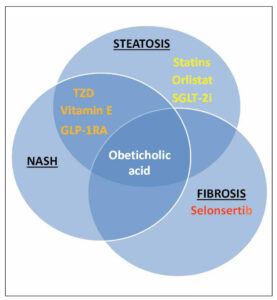
FIGURE 2. The main effects of different medications on the main histological components of NAFLD. Statins, orlistat and SGLT-2i are mainly beneficial for hepatic steatosis, and selonsertib, an apoptosis signal-regulating kinase-1 inhibitor for hepatic fibrosis. TZD (e.g. pioglitazone), vitamin E and GLP-1RA seem to be beneficial for both steatosis and NASH. To-date only obeticholic acid was shown to be beneficial for steatosis, NASH and fibrosis. Abbreviations: GLP-1RA, glucagon-like peptide-1 receptor agonists; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; SGLT-2i, sodium-glucose co-transporter 2 inhibitors; TZD, thiazolidinediones.
Since oxidative stress has been implicated in NAFLD pathophysiology, antioxidant medications have been investigated; vitamin E has been recently recommended as off-label therapy in specific NAFLD patients29. Vitamin E ameliorates hepatic biochemical and histological outcomes in NAFLD patients, without, however, improving hepatic fibrosis48,49. Nonetheless, the potential risk of cardiovascular adverse effects and prostate cancer in men hinders the widespread use of vitamin E in the long-term50.
Lipids and lipoproteins are major contributing factors to the evolution and progression of NAFLD. Thus, lipid lowering medications have also been investigated, considering that NAFLD is accompanied with increased cardiovascular risk51. Statins play a key role in the treatment of dyslipidemia and have been proposed for NAFLD treatment52,53. Although, most studies demonstrated a beneficial effect of statins on steatosis and possibly on inflammation, no data support improvement in fibrosis and additionally, studies with paired liver biopsies were small to indicate robust findings52,53. As for the polyunsaturated fatty acids (PUFAs), such as omega-3 fatty acids, which are administered for hypertriglyceridemia, controversial findings related to NAFLD did not favor their use as monotherapy specifically for NAFLD management. The American Association for the study of Liver Diseases recommended omega-3 fatty acids for the management of hypertriglyceridemia in NAFLD patients29,54,55, as proposed for the management of non-NAFLD individuals with hypertriglyceridemia.
Anti-obesity drugs, such as orlistat, were shown to improve hepatic steatosis and possibly inflammation, an effect that is mainly driven by weight reduction56. However, current anti-obesity medications, as monotherapy, cannot result in weight loss greater than 10%, which is, as mentioned above, necessary to improve hepatic fibrosis9.
Farnesoid X receptor (FXR) is a nuclear receptor transcription factor related to genes that regulate bile acids, glucose and lipid metabolism. The FXR agonist, obeticholic acid, showed beneficial effects in patients with NASH by ameliorating the histological parameters of NAFLD, including fibrosis57. However, its adverse effects, pruritus and elevation of low-density lipoprotein cholesterol, may limit the extensive use of obeticholic acid57, which is currently in a phase III clinical trial of NASH patients.
Another pathogenetic pathway being investigated for potential therapeutic impact is gut microbiota. Prebiotics and probiotics have been considered for the prevention and treatment of NAFLD, and a latent effect of these supplements has been shown in patients with NAFLD as opposed to non-NAFLD individuals58,59. However, there is a controversy yet regarding the diversity of microbial supplements and the unique gut microbiota of each patient, which may be altered in a dynamic fashion in the long-term58. All these currently limit the use of prebiotics and probiotics for the treatment of NAFLD.
Some medications have already been included in phase I and II clinical trials targeting inflammation pathways [e.g., c-Jun N-terminal kinase (NCT04048876), toll-like receptor 4 antagonist (NCT04480710)]. Furthermore, several studies investigated medications related to apoptosis, which is considered to be a principal step for the progression of NAFL and NASH, but in phase III clinical trials none presented beneficial effects on fibrosis or cirrhosis60,61. Given the complexity of the mechanisms leading to fibrosis and emphasizing the difficulty in treating this stage of NAFLD, C-C chemokine receptor 2/5 antagonists (e.g. cenicriviroc) and galectin-3 inhibitors demonstrated promising outcomes, although they did not meet the primary endpoints in the respective clinical trials62,63.
4.1. Anti-diabetic medications in the management of NAFLD
A variety of anti-diabetic medications have been investigated for the treatment of NAFLD64. As T2DM and IR are principally associated with NAFLD pathogenesis, hypoglycemic medications showed promising results and some of them are already included in phase III clinical trials.
In the thiazolidinedione class, pioglitazone, an agonist of peroxisome proliferator-activated receptor gamma (PPAR-γ) controlling glucose and lipid metabolism, indicated histological amelioration with regard to steatosis and NASH65,66. Pioglitazone has been also recommended as off-label treatment in some NASH patients by most guidelines29; however, cautious administration is warranted in the coexistence of heart failure, bladder cancer and osteoporosis, which are the main contraindications of pioglitazone in NASH patients29.
Glucagon-like peptide-1 receptor agonists (GLP-1RA) participate in postprandial insulin release and are approved medications for the treatment of T2DM and some of them (e.g. liraglutide, semaglutide) for the treatment of obesity67. Liraglutide, as well as, semaglutide have shown beneficial outcomes in phase II clinical trials both by achieving NASH resolution with no worsening of fibrosis, without, however, improving fibrosis68,69. Semaglutide is currently on a phase III clinical trial (NCT04822181).
Sodium-glucose co-transporter 2 (SGLT-2) is expressed in the kidney and it is responsible for the reabsorption of glucose70. The inhibition of SGLT-2 reduces plasma glucose by increasing glucose excretion via urine70. In a randomized double-blinded clinical trial dapagliflozin, a SGLT-2 inhibitor (SGLT-2i) in combination with omega-3 carboxylic acids decreased hepatic fat, measured by MRI proton density fat fraction (MRI-PDFF) compared to placebo, while dapagliflozin alone reduced liver function tests and apoptotic biomarkers71. Additionally, dapagliflozin ameliorated liver steatosis in studies used TE and CT with a concomitant reduction in liver function tests72,73.
A phase III clinical trial with dapagliflozin and its effect on NASH is ongoing (NCT03723252). Another SGLT-2i with potential beneficial effects on NAFLD is empagliflozin. Compared with the control group, empagliflozin demonstrated significant improvement in hepatic fat content assessed either by MRS or MRI-PDFF74,75. Similar results were shown for canagliflozin that decreased intra-hepatic fat accumulation based on MRI techniques76,77. Thus, SGLT-2i may be proven significant for the management of NAFLD, beyond their beneficial effects on T2DM, heart failure and chronic kidney disease78.
The above considering, Figure 2 summarizes the main effect of different medications on the main histological components of NAFLD13,14. In summary, statins, orlistat and SGLT-2i are mainly beneficial for hepatic steatosis, and selonsertib, an apoptosis signal-regulating kinase-1 inhibitor for hepatic fibrosis. TZD (e.g. pioglitazone), vitamin E and GLP-1RA seem to be beneficial for both steatosis and NASH. To-date only obeticholic acid was shown to be beneficial for steatosis, NASH and fibrosis (Figure 2).
CONCLUSIONS
NAFLD is a disease of high prevalence, which is expected to be further increased in the next decades in parallel with the epidemics of obesity and T2DM79. Its multi-factorial pathogenesis renders the disease highly heterogeneous, since different contributors affect different patients in a dynamic way. Liver biopsy remains the gold standard of its diagnosis and staging, but much research has been performing on noninvasive indices, based on imaging and circulating biomarkers. Treatment of NAFLD remains an unmet clinical need. Despite the promising research results, there is to-date no medications specifically approved for the management of NAFLD. Fibrosis treatment constitutes a major endpoint of most clinical trials, but no specific medication has been approved for it. Considering the complexity of the mechanisms participated in NAFLD evolution, our interest may need focusing on combination treatments. This seems to be rational, since NAFLD is a multiple-hit disease, which may require multiple-hit management, tailored in a personalized approach80.
Funding
This review has been supported by the Hellenic Atherosclerosis Society in the setting of a scholarship for a doctoral dissertation (ID 516 Φ/4, 6-7-2021).
Declarations of interest
None.
REFERENCES
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology (Baltimore, Md). 2016 Jul;64(1):73-84.
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Journal of hepatology. 2016 May;64(6):1388-402.
- Polyzos SA, Kountouras J, Deretzi G, Zavos C, Mantzoros CS. The emerging role of endocrine disruptors in pathogenesis of insulin resistance: a concept implicating nonalcoholic fatty liver disease. Current molecular medicine. 2012 Jan;12(1):68-82.
- Italian Association for the Study of the Liver (AISF). AISF position paper on nonalcoholic fatty liver disease (NAFLD): Updates and future directions. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2017 Jan;49(5):471-83.
- Jarvis H, Craig D, Barker R, Spiers G, Stow D, Anstee QM, et al. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. PLoS medicine [Internet]. 2020 Apr [cited 2020 Apr 30];17(4):e1003100. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7192386/
- Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol. 2020 Jul;73(1):202-9.
- Eslam M, Sanyal AJ, George J. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology. 2020 May;158(7):1999-2014.e1.
- Polyzos SA, Kang ES, Tsochatzis EA, Kechagias S, Ekstedt M, Xanthakos S, et al. Commentary: Nonalcoholic or metabolic dysfunction-associated fatty liver disease? The epidemic of the 21st century in search of the most appropriate name. Metabolism: Clinical and experimental. 2020 Dec;113:154413.
- Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism: clinical and experimental. 2019 Mar;92:82-97.
- Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J Hepatol. 2016 Sep;65(3):589-600.
- Byrne CD, Targher G. NAFLD: A multisystem disease. Journal of hepatology. 2015 Apr;62(1, Supplement):S47-S64.
- Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L, et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology. 2015 Apr;149(2):367-78. e5; quiz e14-5.
- Polyzos SA, Kang ES, Boutari C, Rhee EJ, Mantzoros CS. Current and emerging pharmacological options for the treatment of nonalcoholic steatohepatitis. Metabolism: clinical and experimental. 2020 Oct;111s:154203.
- Mintziori G, Polyzos SA. Emerging and future therapies for nonalcoholic steatohepatitis in adults. Expert opinion on pharmacotherapy. 2016 Oct;17(14):1937-46.
- Day CP, James OF. Steatohepatitis: A tale of two “hits”? Gastroenterology. 1998 Apr;114(4):842-5.
- Polyzos SA, Kountouras J, Zavos C. The multi-hit process and the antagonistic roles of tumor necrosis factor-alpha and adiponectin in non alcoholic fatty liver disease. Hippokratia. 2009 Apr-Jun;13(2):127; author reply 8.
- Polyzos SA, Kountouras J, Mantzoros CS. Adipokines in nonalcoholic fatty liver disease. Metabolism: clinical and experimental. 2016 Aug;65(8):1062-79.
- Donnelly KL, Smith CI, Schwarzenberg SJ, Jessurun J, Boldt MD, Parks EJ. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J Clin Invest. 2005 May;115(5):1343-51.
- Mota M, Banini BA, Cazanave SC, Sanyal AJ. Molecular mechanisms of lipotoxicity and glucotoxicity in nonalcoholic fatty liver disease. Metabolism: clinical and experimental. 2016 Aug;65(8):1049-61.
- Polyzos SA, Kountouras J, Zavos C, Tsiaousi E. The role of adiponectin in the pathogenesis and treatment of non-alcoholic fatty liver disease. Diabetes Obes Metab. 2010 May;12(5):365-83.
- Polyzos SA, Kountouras J, Mantzoros CS. Adipose tissue, obesity and non-alcoholic fatty liver disease. Minerva Endocrinol. 2017 Jun;42(2):92-108.
- Ye Q, Zou B, Yeo YH, Li J, Huang DQ, Wu Y, et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020 Aug;5(8):739-52.
- Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol. 2019 Oct;71(4):793-801.
- Mantovani A, Byrne CD, Bonora E, Targher G. Nonalcoholic fatty liver disease and risk of incident type 2 diabetes: A Meta-analysis. Diabetes Care. 2018 Feb;41(2):372-82.
- Jiang W, Wu N, Wang X, Chi Y, Zhang Y, Qiu X, et al. Dysbiosis gut microbiota associated with inflammation and impaired mucosal immune function in intestine of humans with non-alcoholic fatty liver disease. Sci Rep. 2015 Feb;5:8096.
- Boursier J, Mueller O, Barret M, Machado M, Fizanne L, Araujo-Perez F, et al. The severity of nonalcoholic fatty liver disease is associated with gut dysbiosis and shift in the metabolic function of the gut microbiota. Hepatology (Baltimore, Md). 2016 Mar;63(3):764-75.
- Eslam M, Valenti L, Romeo S. Genetics and epigenetics of NAFLD and NASH: Clinical impact. J Hepatol. 2018 Feb;68(2):268-79.
- Polyzos SA, Mantzoros CS. An update on the validity of irisin assays and the link between irisin and hepatic metabolism. Metabolism: clinical and experimental. 2015 Sep;64(9):937-42.
- Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology (Baltimore, Md). 2018 Jan;67(1):328-57.
- Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology (Baltimore, Md). 2005 Jun;41(6):1313-21.
- Polyzos SA, Kountouras J, Zavos C, Deretzi G. Nonalcoholic fatty liver disease: multimodal treatment options for a pathogenetically multiple-hit disease. J Clin Gastroenterol. 2012 Apr;46(4):272-84.
- Polyzos SA, Mantzoros CS. Necessity for timely noninvasive diagnosis of nonalcoholic fatty liver disease. Metabolism: clinical and experimental. 2014 Feb;63(2):161-7.
- Bril F, Ortiz-Lopez C, Lomonaco R, Orsak B, Freckleton M, Chintapalli K, et al. Clinical value of liver ultrasound for the diagnosis of nonalcoholic fatty liver disease in overweight and obese patients. Liver Int. 2015 Sep;35(9):2139-46.
- Fishbein M, Castro F, Cheruku S, Jain S, Webb B, Gleason T, et al. Hepatic MRI for fat quantitation: its relationship to fat morphology, diagnosis, and ultrasound. J Clin Gastroenterol. 2005 Aug;39(7):619-25.
- Bohte AE, van Werven JR, Bipat S, Stoker J. The diagnostic accuracy of US, CT, MRI and 1H-MRS for the evaluation of hepatic steatosis compared with liver biopsy: a meta-analysis. Eur Radiol 2011 Jan;21(1):87-97.
- Huwart L, Sempoux C, Vicaut E, Salameh N, Annet L, Danse E, et al. Magnetic resonance elastography for the noninvasive staging of liver fibrosis. Gastroenterology. 2008 Jul;135(1):32-40.
- Talwalkar JA, Kurtz DM, Schoenleber SJ, West CP, Montori VM. Ultrasound-based transient elastography for the detection of hepatic fibrosis: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2007 Oct;5(10):1214-20.
- Hsu C, Caussy C, Imajo K, Chen J, Singh S, Kaulback K, et al. Magnetic Resonance vs Transient Elastography Analysis of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin Gastroenterol Hepatol. 2019 Mar;17(4):630-7.e8.
- Fedchuk L, Nascimbeni F, Pais R, Charlotte F, Housset C, Ratziu V. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment Pharmacol Ther. 2014 Nov;40(10):1209-22.
- He L, Deng L, Zhang Q, Guo J, Zhou J, Song W, et al. Diagnostic Value of CK-18, FGF-21, and Related Biomarker Panel in Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Biomed Res Int [Internet]. 2017 [cited 2017 Feb 23];2017:9729107. Available from: https://pubmed.ncbi.nlm.nih.gov/28326329/
- Xiao G, Zhu S, Xiao X, Yan L, Yang J, Wu G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology (Baltimore, Md) 2017 Nov;66(5):1486-501.
- Ajmera V, Loomba R. Imaging biomarkers of NAFLD, NASH, and fibrosis. Molecular metabolism [Internet]. 2021 Aug [cited 2021 Jan 15];50:101167. Available from: https://pubmed.ncbi.nlm.nih.gov/33460786/
- Fujii H, Enomoto M, Fukumoto S, Kimura T, Nadatani Y, Takashima S, et al. Validation of a two-step approach combining serum biomarkers and liver stiffness measurement to predict advanced fibrosis. JGH Open [Internet]. 2021 Jun [cited 2021 Jun 10];5(7):801-8. Available from: https://pubmed.ncbi.nlm.nih.gov/34263075/
- Leoni S, Tovoli F, Napoli L, Serio I, Ferri S, Bolondi L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J Gastroenterol. 2018 Aug;24(30):3361-73.
- Golabi P, Locklear CT, Austin P, Afdhal S, Byrns M, Gerber L, et al. Effectiveness of exercise in hepatic fat mobilization in non-alcoholic fatty liver disease: Systematic review. World J Gastroenterol. 2016 Jul;22(27):6318-27.
- Keating SE, Hackett DA, George J, Johnson NA. Exercise and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J Hepatol. 2012 Jul;57(1):157-66.
- Fakhry TK, Mhaskar R, Schwitalla T, Muradova E, Gonzalvo JP, Murr MM. Bariatric surgery improves nonalcoholic fatty liver disease: a contemporary systematic review and meta-analysis. Surg Obes Relat. 2019 Mar;15(3):502-11.
- Amanullah I, Khan YH, Anwar I, Gulzar A, Mallhi TH, Raja AA. Effect of vitamin E in non-alcoholic fatty liver disease: a systematic review and meta-analysis of randomised controlled trials. Postgrad Med J. 2019 Nov;95(1129):601-11.
- Bril F, Biernacki DM, Kalavalapalli S, Lomonaco R, Subbarayan SK, Lai J, et al. Role of Vitamin E for Nonalcoholic Steatohepatitis in Patients With Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care. 2019 Aug;42(8):1481-8.
- Miller ER, 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005 Jan;142(1):37-46.
- Polyzos SA, Kechagias S, Tsochatzis EA. Review article: non-alcoholic fatty liver disease and cardiovascular diseases: associations and treatment considerations. Alimentary pharmacology & therapeutics. 2021 Aug;54(8):1013-25.
- Tziomalos K, Athyros VG, Paschos P, Karagiannis A. Nonalcoholic fatty liver disease and statins. Metabolism: clinical and experimental. 2015 Oct;64(10):1215-23.
- Athyros VG, Alexandrides TK, Bilianou H, Cholongitas E, Doumas M, Ganotakis ES, et al. The use of statins alone, or in combination with pioglitazone and other drugs, for the treatment of non-alcoholic fatty liver disease/non-alcoholic steatohepatitis and related cardiovascular risk. An Expert Panel Statement. Metabolism: clinical and experimental. 2017 Jun;71:17-32.
- Parker HM, Johnson NA, Burdon CA, Cohn JS, O’Connor HT, George J. Omega-3 supplementation and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J Hepatol. 2012 Apr;56(4):944-51.
- Sanyal AJ, Abdelmalek MF, Suzuki A, Cummings OW, Chojkier M. No significant effects of ethyl-eicosapentanoic acid on histologic features of nonalcoholic steatohepatitis in a phase 2 trial. Gastroenterology. 2014 Aug;147(2):377-84.e1.
- Harrison SA, Fecht W, Brunt EM, Neuschwander-Tetri BA. Orlistat for overweight subjects with nonalcoholic steatohepatitis: A randomized, prospective trial. Hepatology (Baltimore, Md). 2009 Jan;49(1):80-6.
- Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet (London, England). 2015 Mar;385(9972):956-65.
- Loman BR, Hernández-Saavedra D, An R, Rector RS. Prebiotic and probiotic treatment of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Nutr Rev. 2018 Nov;76(11):822-39.
- Sharpton SR, Maraj B, Harding-Theobald E, Vittinghoff E, Terrault NA. Gut microbiome-targeted therapies in nonalcoholic fatty liver disease: a systematic review, meta-analysis, and meta-regression. Am J Clin Nutr. 2019 Jul;110(1):139-49.
- Harrison SA, Goodman Z, Jabbar A, Vemulapalli R, Younes ZH, Freilich B, et al. A randomized, placebo-controlled trial of emricasan in patients with NASH and F1-F3 fibrosis. J Hepatol. 2020 May;72(5):816-27.
- Harrison SA, Wong VW, Okanoue T, Bzowej N, Vuppalanchi R, Younes Z, et al. Selonsertib for patients with bridging fibrosis or compensated cirrhosis due to NASH: Results from randomized phase III STELLAR trials. J Hepatol. 2020 Jul;73(1):26-39.
- Friedman SL, Ratziu V, Harrison SA, Abdelmalek MF, Aithal GP, Caballeria J, et al. A randomized, placebo-controlled trial of cenicriviroc for treatment of nonalcoholic steatohepatitis with fibrosis. Hepatology (Baltimore, Md) . 2018 May;67(5):1754-67.
- Chalasani N, Abdelmalek MF, Garcia-Tsao G, Vuppalanchi R, Alkhouri N, Rinella M, et al. Effects of Belapectin, an Inhibitor of Galectin-3, in Patients With Nonalcoholic Steatohepatitis With Cirrhosis and Portal Hypertension. Gastroenterology. 2020 Apr;158(5):1334-45.e5.
- Blazina I, Selph S. Diabetes drugs for nonalcoholic fatty liver disease: a systematic review. Systematic reviews. 2019 Nov;8(1):295.
- Belfort R, Harrison SA, Brown K, Darland C, Finch J, Hardies J, et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med. 2006 Nov;355(22):2297-307.
- Cusi K, Orsak B, Bril F, Lomonaco R, Hecht J, Ortiz-Lopez C, et al. Long-Term Pioglitazone Treatment for Patients With Nonalcoholic Steatohepatitis and Prediabetes or Type 2 Diabetes Mellitus: A Randomized Trial. Ann Intern Med. 2016 Sep;165(5):305-15.
- MacDonald PE, El-Kholy W, Riedel MJ, Salapatek AM, Light PE, Wheeler MB. The multiple actions of GLP-1 on the process of glucose-stimulated insulin secretion. Diabetes. 2002 Dec;51 Suppl 3:S434-42.
- Armstrong MJ, Gaunt P, Aithal GP, Barton D, Hull D, Parker R, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet (London, England). 2016 Feb;387(10019):679-90.
- Newsome PN, Buchholtz K, Cusi K, Linder M, Okanoue T, Ratziu V, et al. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N Engl J Med. 2021 Mar;384(12):1113-24.
- Mudaliar S, Polidori D, Zambrowicz B, Henry RR. Sodium-Glucose Cotransporter Inhibitors: Effects on Renal and Intestinal Glucose Transport: From Bench to Bedside. Diabetes Care. 2015 Dec;38(12):2344-53.
- Eriksson JW, Lundkvist P, Jansson PA, Johansson L, Kvarnström M, Moris L, et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: a double-blind randomised placebo-controlled study. Diabetologia. 2018 Sep;61(9):1923-34.
- Kurinami N, Sugiyama S, Yoshida A, Hieshima K, Miyamoto F, Kajiwara K, et al. Dapagliflozin significantly reduced liver fat accumulation associated with a decrease in abdominal subcutaneous fat in patients with inadequately controlled type 2 diabetes mellitus. Diabetes Res Clin Pract. 2018 Aug;142:254-63.
- Shimizu M, Suzuki K, Kato K, Jojima T, Iijima T, Murohisa T, et al. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes Metab. 2019 Feb;21(2):285-92.
- Kahl S, Gancheva S, Straßburger K, Herder C, Machann J, Katsuyama H, et al. Empagliflozin Effectively Lowers Liver Fat Content in Well-Controlled Type 2 Diabetes: A Randomized, Double-Blind, Phase 4, Placebo-Controlled Trial. Diabetes Care. 2020 Feb;43(2):298-305.
- Kuchay MS, Krishan S, Mishra SK, Farooqui KJ, Singh MK, Wasir JS, et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes care. 2018 Aug;41(8):1801-8.
- Cusi K, Bril F, Barb D, Polidori D, Sha S, Ghosh A, et al. Effect of canagliflozin treatment on hepatic triglyceride content and glucose metabolism in patients with type 2 diabetes. Diabetes Obes Metab. 2019 Apr;21(4):812-21.
- Inoue M, Hayashi A, Taguchi T, Arai R, Sasaki S, Takano K, et al. Effects of canagliflozin on body composition and hepatic fat content in type 2 diabetes patients with non-alcoholic fatty liver disease. J Diabetes Investig. 2019 Jul;10(4):1004-11.
- Makri ES, Goulas A, Polyzos SA. Sodium-glucose co-transporter 2 inhibitors in nonalcoholic fatty liver disease. Eur J Pharmacol. 2021 Sep;907:174272.
- Makri E, Goulas A, Polyzos SA. Epidemiology, Pathogenesis, Diagnosis and Emerging Treatment of Nonalcoholic Fatty Liver Disease. Arch Med Res. 2021 Jan;52(1):25-37.
- Polyzos SA, Kountouras J, Anastasiadis S, Doulberis M, Katsinelos P. Nonalcoholic fatty liver disease: Is it time for combination treatment and a diabetes-like approach? Hepatology (Baltimore, Md). 2018 Jul;68(1):389.